Suspected Stroke Algorithm

In the event of a suspected stroke, follow these stroke protocol guidelines. For more free resources like our ACLS stroke algorithm guide, explore other online articles to refresh your life-saving skills.
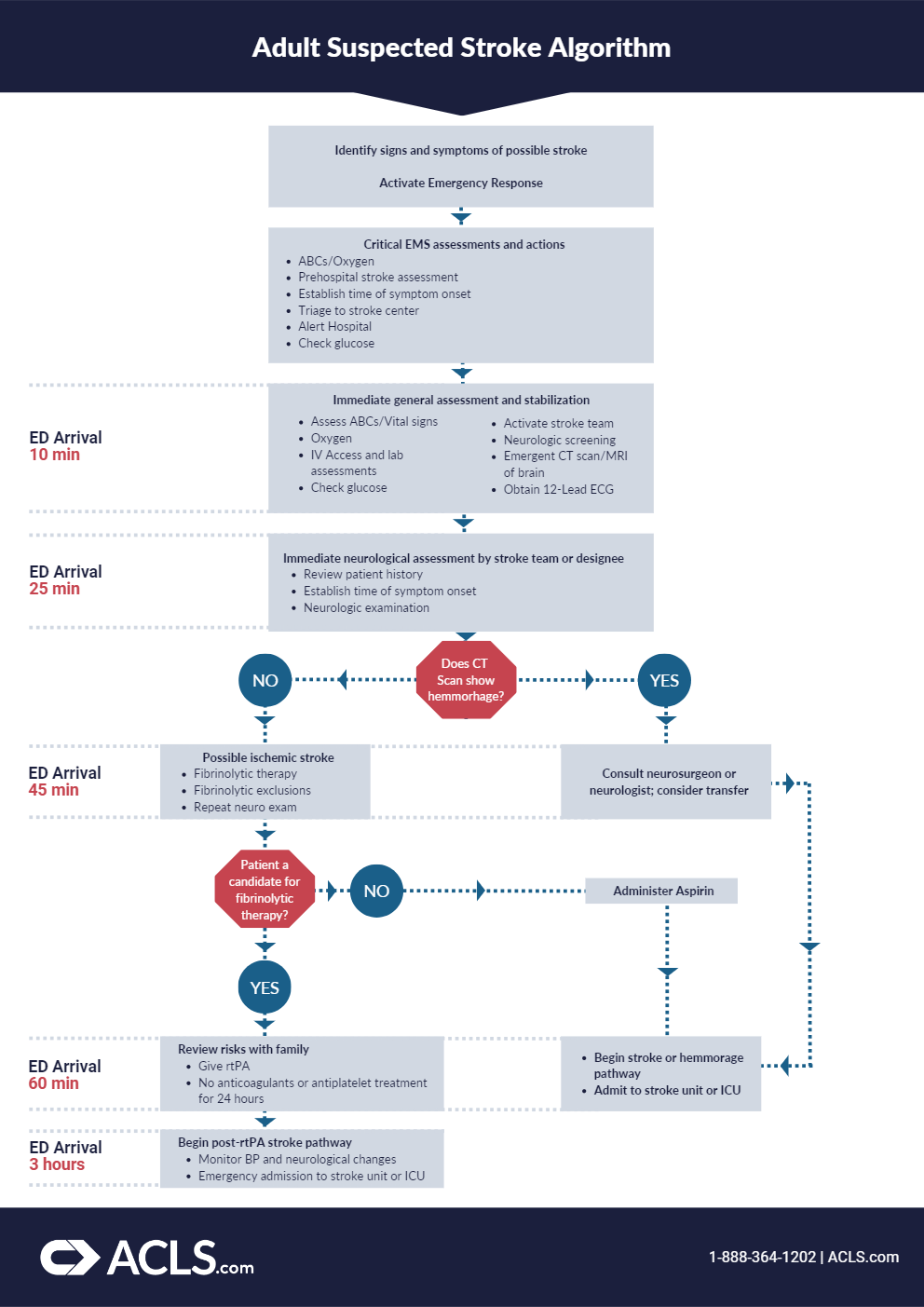
- Identify signs and symptoms of possible stroke and activate emergency response. Observe the patient for signs of a stroke. Use F-A-S-T to remember the warning signs: facial drooping, arm weakness, speech difficulties, and time. Call 911 immediately, or have someone else call, to activate the emergency response system.
- Critical EMS assessments and actions. Support ABCs, giving the patient oxygen if needed, and perform a prehospital stroke assessment. Determine the time of stroke onset and triage the patient to a stroke center, alerting the hospital in advance so they can activate the stroke team. Consider directing the patient to CT scan, and if possible, check glucose levels.
- Immediate general assessment and stabilization. Once the patient has arrived at the emergency department, and within 10 minutes of arrival, assess the vitals, providing oxygen if the patient is hypoxemic. Obtain IV access, run labs, check glucose, activate the stroke team, perform neurologic screening with emergent CT scan or MRI of the brain, and obtain a 12-lead ECG.
- Immediate neurologic assessment by stroke team or designee. Within 25 minutes of arrival at the emergency department, the stroke team or designee should review the patient’s history, establish a timeline of symptom onset, and perform a neurologic examination using either the NIH Stroke Scale or the Canadian Neurological Scale.
- Does CT scan show hemorrhage? Determine whether or not the CT scan shows hemorrhage within 45 minutes of the patient’s arrival at the emergency department.
- Probable acute ischemic stroke; consider fibrinolytic therapy. If the CT scan shows no sign of hemorrhage, it is probable that the patient experienced an ischemic stroke and is a candidate for fibrinolytic therapy. Check for fibrinolytic exclusions such as significant head trauma or stroke in the previous 3 months, history of intracranial hemorrhage, elevated blood pressure, active internal bleeding, or a blood glucose concentration less than 50 milligrams per deciliter. Then repeat the neurologic exam.
- Consult a neurologist or neurosurgeon. If the CT scan indicates hemorrhage, consult neurologists and neurosurgeons, and begin the stroke or hemorrhage pathway.
- Administer aspirin. If the patient is not a candidate for fibrinolytic therapy, administer aspirin and begin the stroke or hemorrhage pathway.
- Begin stroke or hemorrhage pathway. Begin the stroke or hemorrhage pathway and admit the patient to the stroke unit or intensive care unit.
- Review risks/benefits with the patient and family. If the patient remains a candidate for fibrinolytic therapy, review the risks and benefits of the therapy with the patient and their family within 1 hour of arrival and 3 hours of symptom onset. If they agree to the treatment, administer rtPA and do not give the patient anticoagulants or antiplatelets for 24 hours.
- Begin post-rtPA stroke pathway. Begin the post-rtPA stroke pathway within 3 hours of patient arrival to the emergency department. Admit the patient into the stroke unit or intensive care unit and aggressively monitor blood pressure and neurologic deterioration.